
Gavi’s High-Impact Countries: A Critical Step Toward global Immunization Goals
In a bold move to address the global immunization gap,Gavi,the vaccine Alliance,has designated a group of nations as “high-impact countries.” These countries—Democratic Republic of Congo, Ethiopia, India, Nigeria, and Pakistan—are pivotal to achieving Gavi’s enterprising objectives for the 2021–2025 strategic period. Together, they represent 26% of the world’s population, 48% of global births, and a staggering 56% of all zero-dose children in Gavi-eligible nations.
National success, Subnational Challenges
Table of Contents
- National success, Subnational Challenges
- Protecting Vaccination Amid Instability
- Driving Progress Through Partnerships
- Key Insights: High-Impact Countries
- Zero-Dose Children: A Persistent Challenge
- Funding and Co-Financing Efforts
- Key Data at a Glance
- The Road Ahead
- Interview: Protecting Vaccination Amid Instability
- Editor: Can you explain the key pillars of Gavi’s 2021–2025 strategy in high-impact countries?
- Editor: How is Gavi addressing subnational challenges in vaccination programs?
- Editor: What are the key insights regarding high-impact countries?
- Editor: Can you elaborate on the issue of zero-dose children in these countries?
- editor: How is Gavi supporting these countries financially?
- Editor: What are the next steps in reducing zero-dose children globally?
- Editor: Thank you for sharing these insights.
The impact of Gavi’s efforts in these countries is undeniable. Between 2000 and 2022, 481 million children were immunized through routine vaccination programs supported by Gavi, accounting for 45% of all children vaccinated under the alliance’s initiatives. In 2021–2022 alone, 69 million children received life-saving vaccines, preventing an estimated 6.8 million future deaths.
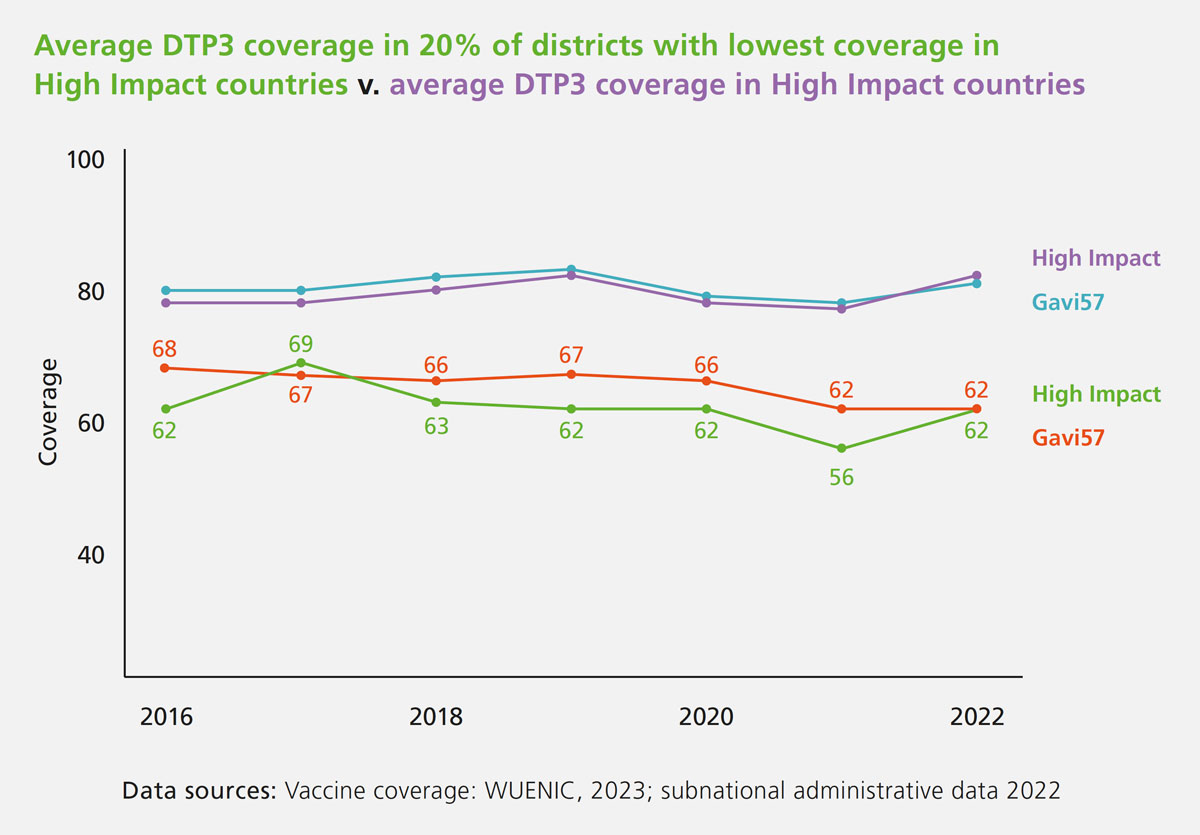
However, the story at the subnational level is more complex. Districts with low vaccination coverage continue to lag behind. In 2022,the 20% of districts with the lowest coverage achieved a 62% rate for the third dose of the diphtheria,tetanus,and pertussis vaccine (DTP3). While this marks an betterment from 2021, it remains significantly below the 82% average recorded across all high-impact countries.
Protecting Vaccination Amid Instability
High-impact countries often grapple with political and economic instability, programmatic risks, and humanitarian crises, including active conflicts and refugee populations. These challenges are particularly pronounced at the subnational level, where vaccination programs face heightened risks.To address these barriers, Gavi’s 2021–2025 strategy focuses on three key pillars:
- Equity-driven objectives: Targeting zero-dose children and underserved communities.
- Differentiated approaches: Tailoring interventions to the unique needs of Gavi-eligible countries.
- Programmatic sustainability: Ensuring long-term resilience of immunization programs.
The alliance is also committed to strengthening political commitment to vaccination at both national and subnational levels, recognizing its critical role in achieving equitable immunization coverage.
Driving Progress Through Partnerships
During the 2021–2025 period, Gavi has implemented geographically targeted interventions in 28% of districts with the highest proportions of zero-dose children. This shift toward subnational programming leverages diverse implementation methods, including the use of common funds, memorandums of understanding (MoUs) with subnational entities, and direct payments to local authorities.
Key Insights: High-Impact Countries
| Metric | value |
|——————————–|——————————-|
| Population (2022) | 2,093,710,000 |
| Zero-dose children (2022) | 56% of Gavi-eligible countries|
| Children vaccinated (2000–2022)| 481 million |
| Future deaths averted (2000–2022)| 6.8 million |The global effort to vaccinate children and reduce the number of zero-dose children has seen important progress,but challenges remain. Five countries—India,Pakistan,Nigeria,Ethiopia,and the Democratic Republic of Congo (DRC)—account for 26.3% of the world’s population, with a combined population of over 2 billion people. These nations are also home to 28% of the world’s zero-dose children, with 943 high-concentration districts identified globally.
Zero-Dose Children: A Persistent Challenge
Zero-dose children, those who have not received any routine vaccinations, are concentrated in specific regions. In the DRC, 136 out of 519 health zones report high numbers of zero-dose children, while Ethiopia has 477 woredas out of 1,110 affected. India,with its vast population,has 143 districts out of 766 identified as high-risk areas. Nigeria and Pakistan also face significant challenges, with 100 local administrative zones and 87 districts, respectively, reporting high concentrations of zero-dose children.
Funding and Co-Financing Efforts
To address these challenges, Gavi, the Vaccine Alliance, has disbursed a total of $10.2 billion,representing 26% of its overall funding. The DRC has received $1.77 billion, Ethiopia $1.7 billion, and India $1.67 billion. Nigeria and Pakistan have been allocated $2.3 billion and $3.3 billion, respectively. Additionally,co-financing payments from eligible countries since 2008 total $781.4 million, with Nigeria contributing $381.1 million and Pakistan $263.4 million. The DRC and Ethiopia have also contributed $80.5 million and $56.4 million, respectively.
Key Data at a Glance
The table below summarizes the key statistics for these five countries:
| Country | Population | Zero-Dose districts | Funding Received | Co-Financing Payments |
|—————|—————-|————————-|———————-|—————————|
| India | 1,417,000,000 | 143 out of 766 | $1.67 billion | – |
| Pakistan | 235,800,000 | 87 out of 158 | $3.3 billion | $263.4 million |
| Nigeria | 218,500,000 | 100 out of 774 | $2.3 billion | $381.1 million |
| Ethiopia | 123,400,000 | 477 out of 1,110 | $1.7 billion | $56.4 million |
| DRC | 99,010,000 | 136 out of 519 | $1.77 billion | $80.5 million |
The Road Ahead
While significant funding has been allocated, the distribution of resources and the identification of high-risk areas remain critical. Addressing the needs of zero-dose children in these regions requires continued collaboration between governments,organizations like Gavi,and local communities. The focus must remain on ensuring that every child, regardless of location, has access to life-saving vaccines.
The fight against preventable diseases is far from over, but with sustained efforts, the goal of reducing zero-dose children globally is within reach.
Interview: Protecting Vaccination Amid Instability
Editor: Can you explain the key pillars of Gavi’s 2021–2025 strategy in high-impact countries?
Guest: Absolutely. Gavi’s 2021–2025 strategy focuses on three critical pillars to address challenges in high-impact countries. First, there are equity-driven objectives, which target zero-dose children and underserved communities. Second,we employ differentiated approaches,tailoring interventions to the unique needs of Gavi-eligible countries.Lastly, we emphasize programmatic sustainability to ensure the long-term resilience of immunization programs.
Editor: How is Gavi addressing subnational challenges in vaccination programs?
Guest: Subnational challenges are significant,especially in areas with political instability,conflict,and refugee populations. Gavi has implemented geographically targeted interventions in 28% of districts with the highest proportions of zero-dose children. We’ve shifted toward subnational programming, leveraging methods like common funds, memorandums of understanding (MoUs) with subnational entities, and direct payments to local authorities.
Editor: What are the key insights regarding high-impact countries?
Guest: High-impact countries,which include India,Pakistan,Nigeria,Ethiopia,and the Democratic Republic of Congo (DRC),face unique challenges. These nations account for 26.3% of the global population and 28% of the world’s zero-dose children. Despite significant progress, such as vaccinating 481 million children and averting 6.8 million future deaths as 2000, challenges like zero-dose children persist in specific regions.
Editor: Can you elaborate on the issue of zero-dose children in these countries?
Guest: Certainly. zero-dose children are concentrated in specific regions within these countries. For example, in the DRC, 136 out of 519 health zones report high numbers of zero-dose children. Similarly, Ethiopia has 477 woredas out of 1,110 affected. India, with its vast population, has 143 districts out of 766 identified as high-risk. Nigeria and Pakistan also face significant challenges, with 100 and 87 high-concentration districts, respectively.
editor: How is Gavi supporting these countries financially?
Guest: Gavi has disbursed a total of $10.2 billion, representing 26% of its overall funding. The DRC has received $1.77 billion, Ethiopia $1.7 billion, and India $1.67 billion. Nigeria and Pakistan have been allocated $2.3 billion and $3.3 billion, respectively. Additionally, co-financing payments from eligible countries since 2008 total $781.4 million, with Nigeria and Pakistan contributing considerably.
Editor: What are the next steps in reducing zero-dose children globally?
Guest: The road ahead requires continued collaboration between governments, organizations like Gavi, and local communities. We must focus on distributing resources efficiently and identifying high-risk areas. Our goal is to ensure every child, irrespective of location, has access to life-saving vaccines. With sustained efforts, reducing the number of zero-dose children globally is within reach.
Editor: Thank you for sharing these insights.
Guest: You’re welcome. It’s crucial to highlight these efforts and challenges as we work toward equitable immunization coverage worldwide.


{kind=link}